We only consider nonprofit organizations implementing interventions that are backed by rigorous evidence of impact and that are cost-effective. Furthermore, we define high-impact nonprofits as those that consistently achieve measurable, evidence-supported, and sustainable improvements in the lives of individuals, which would not have happened without their contribution. We support these organizations to ensure that every dollar invested in them can go the furthest in generating positive outcomes and reduce suffering. Two key questions we examine are:
- Is there evidence of impact of the intervention when implemented by the organization?
- Is the organization able to implement the intervention at a cost-effective rate?
Since interventions are implemented by the nonprofit organizations we recommended, there is overlap between the intervention and organization spheres. Therefore, as part of our consideration of nonprofits to recommend, we pay close attention to an intervention’s: scale, depth and durability.
From an organizational perspective the questions to assess these elements are formulated as:
- Does the organization have the ability to operate at scale?
- Does the organization’s work reflect depth by addressing multiple MPI indicators?
- Is there evidence that the intervention delivered by the organization has durable impact?
In our evaluation and monitoring of nonprofit organizations, we take into account these three dimensions and consider how organizations can achieve similar levels of impact through different strategies. We illustrate this in Box 1.
| Box 1. Organizational impact across scale, depth, and durability | |
| Examples: | |
|
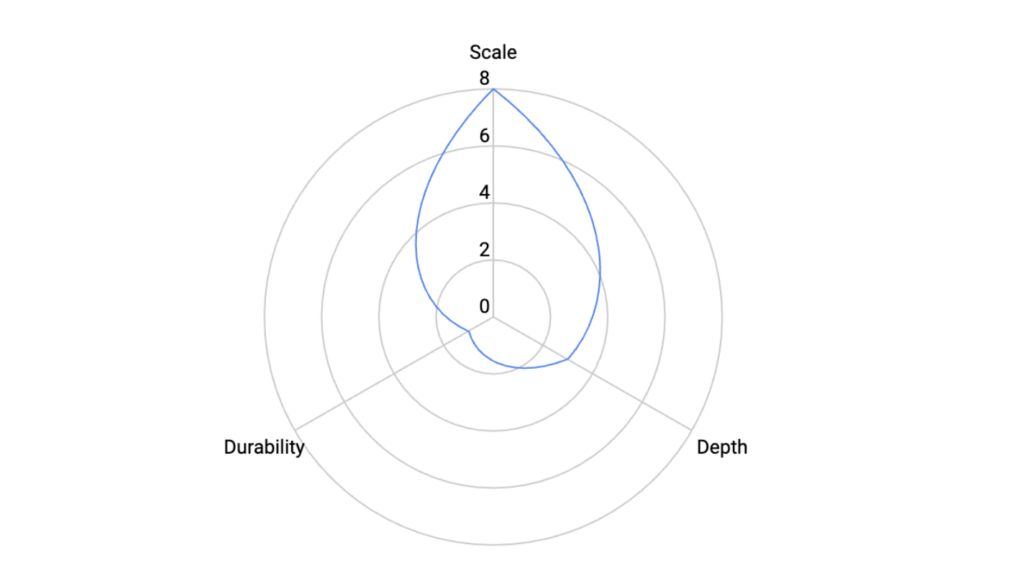
1. Nonprofit A provides a narrow intervention that it distributes to millions of people. The intervention prevents people from contracting disease X but it cannot help beneficiaries in other ways. The intervention must be repeated every year. Their impact can be visualized as follows:
|
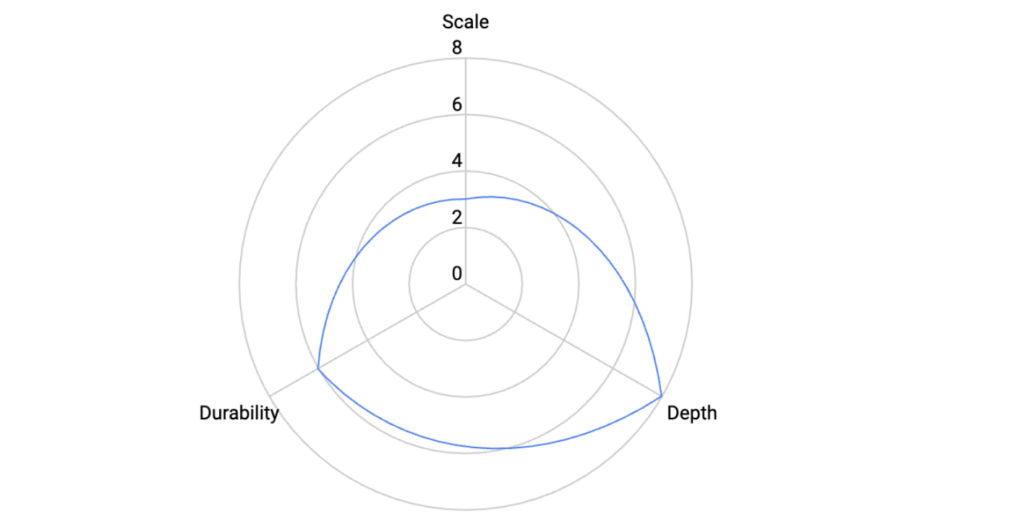
2. Nonprofit B provides an educational programme that supports beneficiaries in various aspects of their life. The intervention has proven to increase wellbeing, income and health of beneficiaries. The cost of the intervention is high and the organization cannot directly reach vast amounts of people directly. A longitudinal study showed intergenerational effects of the intervention. Their impact can be visualized as follows: |
 |
 |
Even highly effective interventions require organizations with the capacity to implement them broadly and reliably. We therefore assess an organizations’ capacity to operate at scale by looking at the number of people reached each year and whether the organization meets its yearly targets. A strong track record of delivery shows that the organization can reach large populations consistently and reliably. We classify organizations into three levels. Low scale means reaching 100,000 to 1 million people per year. Medium scale means more than 1 million to 2 million. High scale means more than 2 million. These thresholds reflect our experience with the types of organizations we recommend and are consistent with broader frameworks on organizational maturity and absorptive capacity.
In addition to assessing scale, depth, and durability, we also consider a broader set of elements when evaluating organizations. We prioritize those that operate in The Life You Can Save’s priority geographies. We also assess whether an intervention that is cost-effective in general remains cost-effective when implemented by the organization in its specific context. Beyond this, we examine the following elements:
- Is there evidence of high organizational quality?
- Does the organization uphold beneficiaries’ dignity in their work?
- How is the organization embedded in local systems?
- What is the organization’s funding need?
- What are the risks the organization faces?
Next, we provide details on what each of the above entail.
Assessing organizational quality is essential because even strong, evidence-based interventions require organizations with the leadership, systems, and adaptability to deliver them effectively in real-world contexts. Randomized Controlled Trials and other forms of impact evaluation tell us whether an intervention works, but they do not show whether a particular organization can implement it reliably across different settings. To address this gap, we draw on insights from realist evaluation (Pawson & Tilley, 1997; Deaton & Cartwright, 2017; Vivalt, 2020), which emphasize understanding what works, for whom, and under what circumstances. This lens highlights the importance of context, organizational capabilities, and the mechanisms through which change occurs.
Our assessment of organizational quality focuses on an organization’s impact creation logic—the knowledge, processes, and systems that drive its ability to create and sustain meaningful change (Seelos & Mair, 2017). We evaluate whether organizations demonstrate a deep understanding of the problems they address, align their mission closely with their solutions, and adapt interventions effectively to context. Leadership and team capacity are also central: we look at the stability, experience, and structure of teams, and at whether organizations set and consistently achieve clear milestones.
We assess organizational quality across five main criteria:
- Problem space: Understanding of the problem and its root causes, including socio-political and cultural dynamics.
- Identity space: Alignment between mission, problem, and solutions, and resilience in pursuing long-term goals, and articulation of a clear, well-developed theory of change that links activities to outcomes.
- Solution space: Evidence that interventions are contextually appropriate, adaptable, and supported by strong monitoring and feedback systems (from beneficiaries and partners).
- Team and leadership stability: Depth, experience, and continuity of leadership and staff. We assess whether leadership combines technical expertise with proximity to the communities served, whether decision-making is inclusive, and whether the organization has succession planning to ensure continuity.
- Commitment to learning and improvement: A culture of reflection, adaptation, and transparency, supported by robust monitoring, evaluation, and learning (MEL) systems and strong feedback mechanisms that generate evidence and drive program improvements.
We combine desk research, document review, and interviews with organizational staff, as well as external perspectives from donors and partners, to score organizational quality on a three-point scale (high, medium, low). A high-quality organization shows a strong understanding of the problem, effective and adaptable solutions, stable leadership, and a demonstrated commitment to continuous learning.
Research shows that international development beneficiaries deeply value respect for dignity and that, unfortunately, they are also frequently denied. Even when material needs are met, beneficiaries can come away from interactions with service providers feeling mistreated, ignored, or disempowered. For The Life You Can Save, any charity considered impactful must also be one that respects the dignity, priorities, and agency of those it serves.
The Life You Can Save partners with IDInsight’s Dignity Initiative to integrate dignity in our evaluation framework. IDinsight describes three main pathways to consider when reflecting and operationalising the concept of dignity. These are:
- Equity: Treat beneficiaries as if they were equals and reduce power asymmetries.
- Agency: Give beneficiaries choices and meaningful chances to consent.
- Representation: Offer beneficiaries the chance to be and feel seen by the institution delivering aid.
We assess nonprofits on how well they respect dignity alongside other impact factors in deciding whether to recommend them to donors. In our evaluations, we consider the following criteria:
- Priority: When looking at a nonprofit’s website, reports or listening to a presentation, evaluate whether the service they are providing is something people in the area value and are calling for. Most importantly, how does the charity know this is something people need and want? A respectful nonprofit makes reference to participatory processes of preference elicitation, willingness to pay and transparently discusses trade offs with other priorities.
- Interactions with beneficiaries: A respectful nonprofit references concrete steps taken to ensure that beneficiaries are treated fairly and in the way they wish to be treated. Donors should look out for references to the three pathways in nonprofit’s websites, social media, presentations and reports.
- Culture and People: Internal culture is key to developing respectful interactions both within and outside the organization. Donors should look for examples of concrete steps organizations take to ensure staff are treated with respect.
- Listening and Learning: A highly impactful and respectful organization needs tools and mechanisms to know that they are treating people with respect. A nonprofit that respects people’s dignity mentions ongoing and proactive measurement of beneficiaries’ experiences, feedback mechanisms, and shows a track record of adapting their programs based on these mechanisms.
- Safeguarding: A respectful nonprofit has clear and accessible safeguarding policies in place to protect against harm or misconduct. It provides trusted reporting mechanisms that beneficiaries can use to raise concerns and demonstrates how it acts on them.
- Representation: A respectful nonprofit portrays beneficiaries as active agents in their own lives. It avoids paternalistic or disempowering depictions in its communications and highlights dignity, agency, and equality in how it represents its work.
For interventions to be sustainable, nonprofits must be well connected to the communities and systems in which they operate. We therefore assess how organizations fit within the local ecosystem. This includes looking at whether they are locally led, how they engage with community stakeholders, and the extent to which they collaborate with governments. Organizations that are strongly embedded in their local context are more likely to understand community needs, adapt to challenges, and secure the buy-in needed for lasting impact.
We also assess whether organizations have strategies to strengthen local systems over time. This includes efforts to build government capacity, foster community ownership, or create pathways for markets and institutions to take responsibility for effective solutions. While philanthropy can sometimes create risks of dependency (Easterly, 2006; Moyo, 2009), it can also act as a catalyst for innovation and sustainability when paired with strong system-strengthening strategies (Barder, 2014). We prioritize nonprofits that demonstrate clear, operational strategies for embedding their work in local systems and reducing long-term reliance on external support.
When evaluating a nonprofit, we assess its funding needs to determine whether additional resources are likely to generate significant impact. Our assessment considers several factors:
- Unrestricted funding: We look at what proportion of the organization’s budget is unrestricted. Unrestricted funding is particularly valuable because it gives organizations flexibility to allocate resources where they are most needed, invest in capacity, and adapt to challenges. A low proportion of unrestricted funds signals a high need.
- Reliance on TLYCS and philanthropic funding: We assess whether the organization’s funding base is diversified or overly dependent on The Life You Can Save or philanthropy more broadly. Heavy reliance on a single source can compromise financial stability and autonomy, while a medium level of reliance suggests healthier diversification.
- Funding urgency and runway: We consider whether the organization faces time-sensitive needs where delays in funding could disrupt services or lead to missed opportunities. As part of this, we assess the organization’s financial runway, or how long it can continue operating at its current scale without new resources. A short runway increases urgency and signals greater funding need.
- Capacity to absorb funding: We examine whether the organization has the operational systems, leadership, and scaling plans in place to effectively manage additional resources and deliver impact.
We score organizations on each of these dimensions and then determine whether their overall funding need is high, medium, or low. Organizations with a high funding need, typically combine limited unrestricted funding, medium reliance on philanthropy, pressing financial urgency, and strong capacity to absorb new resources.
As part of our evaluation process, we also consider potential risks that could limit an organization’s ability to deliver services to a high standard and achieve the intended impact. This is a qualitative assessment based on all the evidence and documentation we review, combined with our professional judgment. The goal is not to exclude organizations because they face risks, but to be transparent about possible challenges and to identify areas that may require closer monitoring over time.
In assessing risks, we look at both internal and external factors. Internal risks may include organizational capacity, leadership, or systems that affect implementation. External risks may relate to stakeholder engagement, local or national politics, or other contextual challenges. By weighing these factors carefully, we aim to provide a balanced view of each organization’s strengths as well as the uncertainties that could affect its work. This helps us, and our donors, remain aware of potential vulnerabilities while recognizing the impact these organizations are achieving.

